Evidence-Based Ankyloglossia (Tongue Tie) Part One
There’s so much information and opinions around ‘tongue ties’. As a Breastfeeding Medicine Specialist and IBCLC, this is one of the most common referrals I get.
“Does my baby have a tongue tie?”
“ The Midwife said there might be a problem?”
“My sister’s baby had latching issues and it turned out to be a tongue tie…”
There’s a reason this area is controversial, which I will explain further on. But if you’re diving into the world of “tongue ties”, let’s start with what we know about tongues…
What we know about tongue ties

Incidence of affected babies is 1-3%, some studies quote 4-11%
This is likely based on “classic” or “obvious” tongue ties that have traditionally been detected
Up to 30% of babies will have some assessment or treatment for ankyloglossia and there is over-intervention
There is likely under-intervention in some babies as there is no standardised assessment tool for professionals
As there is no one standardised agreement on what a “tongue tie” actually is, and grading of severity, research is difficult (you’re comparing apples with oranges)
Ongoing research is required in this area, but is difficult and often biased
Intervention is offered by professionals, some who have a significant financial interest in performing procedures
Many families identify with being supported by these professionals after being told “nothing is wrong” and misdiagnosed
So, what is a tongue tie? If you take one thing away from this post, be it this…
A tongue tie is a FUNCTIONAL restriction of the tongue’s movement
Underneath the tongue, linking the tongue to the floor of the mouth, is a normal anatomical attachment called the ‘lingual frenulum’. Everyone has one. Not all lingual frenula look the same. Sometimes, the attachment can be tight so that the tongue is tethered and unable to move adequately. This is a ‘tongue tie’.
If there is no functional restriction, no tethering that is affecting the tongue’s movement to the extent that it’s function is compromised, then there is no tongue tie at all.
What does the tongue ‘do’ in infants? It participates in breastfeeding.
Diagnosis of tongue tie CANNOT be made on appearance. It requires a functional assessment.
A functional assessment involves assessment of breastfeeding by someone who is qualified to assess breastfeeding, and an oral suck assessment.
THE LINGUAL FRENULUM (aka the attachment under the tongue")
Just like everyone’s hands look a little different. So too do ‘lingual frenulums’. There are a variety of normal attachments.
This attachment can be:
Thin and almost transparent (membranous)
Thicker with a layer of mucosa (outer membrane), submucosa (inner membrane)
Very thick with both of the above with some genioglossus muscle
We now know, based on revolutionary work by Dr Nikki Mills, that there is not just a band running along the frenulum. We also know that there is much variation in this and all attachments can be normal.
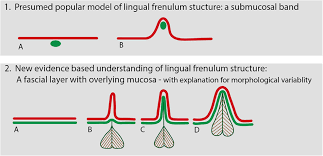
The Lingual Frenulum (Attachment at the underside of the tongue)
Dr Nikki Mills
‘ANTERIOR’ AND ‘POSTERIOR’ ANKYLOGLOSSIA
This terminology is used frequently and anterior (meaning front) refers traditionally to the thin membranous frenulum with attachments towards the tip of the tongue.
Posterior (meaning back) ankyloglossia colloquially really refers to any lingual frenulum that is thought by that practitioner to be causing tethering, that is further back or looks thicker.
WHY I DON’T LIKE THE ANTERIOR AND POSTERIOR TERMINOLOGY
If we know that a tongue tie is a functional restriction of the tongue, then the description of a baby’s lingual attachment focused on appearance (that may be entirely normal) is misleading.
A simple thin frenulum may be called an ‘anterior tongue tie’ where there is no restriction and there may be unnecessary intervention.
A submucosal or thicker ‘posterior tongue tie’ may not be recognised as the ‘classic tongue tie’ and families told that there is no issue when in fact there is indeed functional restriction requiring intervention.
I believe we need to discuss the function primarily and decide if there is a tongue tie and THEN assess the appearance in relation to any procedural intervention.
IF THE TONGUE IS RESTRICTED, WHAT DOES THIS DO?
If the tongue is tethered, this affects fit and hold (baby’s oral attachment to the birthing parent’s nipple).
This can result in:
Maternal nipple pain
Damage to nipple - abrasions, cracks, bleeding
Difficulty attaching to the nipple
Baby winding up at the breast (can be either crying or being shut down and “falling asleep”)
Difficult milk transfer (slowing infant weight gain, longer time mother’s milk supply)
WHAT A TONGUE TIE DOES NOT CAUSE
Speech Problems
Unless severe, there is no association with speech problems later in childhood
This is because the infant mouth grows rapidly in the first few months of life and the frenulum often stretches over time, the mouth is dynamic and changing and minor restriction may have no effect in the future
Dental Problems
There is no evidence that major dental problems occur
evidence based fact 1: when discussing intervention for tongue ties, the evidence relates solely to breastfeeding and there is no evidence that intervening based on appearance alone for bottle feeding, unsettled behaviour, future speech or dental issues will improve outcomes
DIAGNOSIS OF A TONGUE TIE CANNOT BE MADE IF THERE IS POOR FIT AND HOLD AND BREASTFEEDING POSITIONING/ LATCHING
Fit and Hold/ Positioning/ Attachment/ Latch is KING/ QUEEN.
Many Mothers and Babies referred, with appropriate adjustment and support, will find that they are able to feed their babies without pain or issue, and respond to fit and hold intervention alone.
If fit and hold isn’t right, then we can’t entirely tell if there’s a tongue tie. Why? Because ultimately it’s a functional restriction and even an oral assessment won’t ever entirely replicate the tongues’ function when breastfeeding.
Even if there is a tongue tie, if fit and hold/ latch/ attachment isn’t great then there can still be ongoing pain.
EVIDENCE BASED FACT 2: The best outcomes in relation to tongue ties and intervention, relate to COMPREHENSIVE BREASTFEEDING SUPPORT (i.e. fit and hold adjustment).
This makes sense really, as even if you release any tethering and the tongue is moving well, but the baby isn’t stable at the breast or just on the nipple superficially, then there will be pain / fussing at the breast/ issues.